
Written by Lulu, RSEI Educator | Published October 18th, 2024
*Language Note: For this post, we are leaning on existing research around pregnancy and childbirth-related mortality for people in the United States. This research uses gendered language (women, maternal mortality, etc.) that does not account for the fact that not all pregnant people identify as female. We are using language consistent with the broad scientific discourse on this topic, but acknowledge that not all pregnant and parenting people identify as mothers.
It is a well-known and shameful fact that the US has a disproportionately high rate of maternal mortality, especially compared to other industrialized nations. The CDC’s National Center for Health Statistics’ most recent report found the maternal mortality rate to be at 32.9 deaths per 100,000 births in the US. For comparison, in 2022 the number of deaths was 0 in Norway, 1.2 in Switzerland, 3.5 in Australia, 5.5 in the UK, 8.4 in Canada, and 8.8 in Korea. Most concerning are the racial disparities in maternal mortality; for example, Black women in the US are at least three times more likely to die due to a pregnancy-related cause when compared to white women. If you’d like to read more about these disparities and how youth-serving adults can use this information, check out Victoria’s blog post from Aug 2021.
However, if you’ve followed the news on maternal mortality in the US over the last year, you may have noticed some interesting new studies that call into question the data the US has relied on for the past few decades. Researchers poring over the numbers recently have found that the rise in rates in the US has largely been due to a change in the way maternal mortality is measured in this country. This change was gradually introduced state-by-state between 2003 and 2017, and some key elements of the new system reveal why it has led to misclassification of maternal deaths.
Maternal mortality is defined as death due to pregnancy, childbirth, abortion, or related causes. In 1994, the International Classification of Diseases recommended adding a “pregnancy” checkbox to US death certificates. The introduction of the checkbox led to a rapid increase in reported maternal deaths between 2003-2017, but recent studies have found that the checkbox system actually led to some egregious errors: while it did lead to the counting of many deaths that would have otherwise been missed, it also led to overcounting in many circumstances. For example, the system may capture a woman who died in a car accident but happened to be pregnant at the time. Or, as a doctor in Louisiana noted, “When we’re validating the cases, it’s very common that a 70 year old man – somebody checked the pregnancy checkbox and it will appear that that was a pregnancy-associated death when it was more of a clerical error” (NPR).
The image below shows how the checkbox system could lead to potential misclassification:

And this graph shows how the maternal mortality doubled on average after the US adopted the pregnancy checkbox on death certificates:
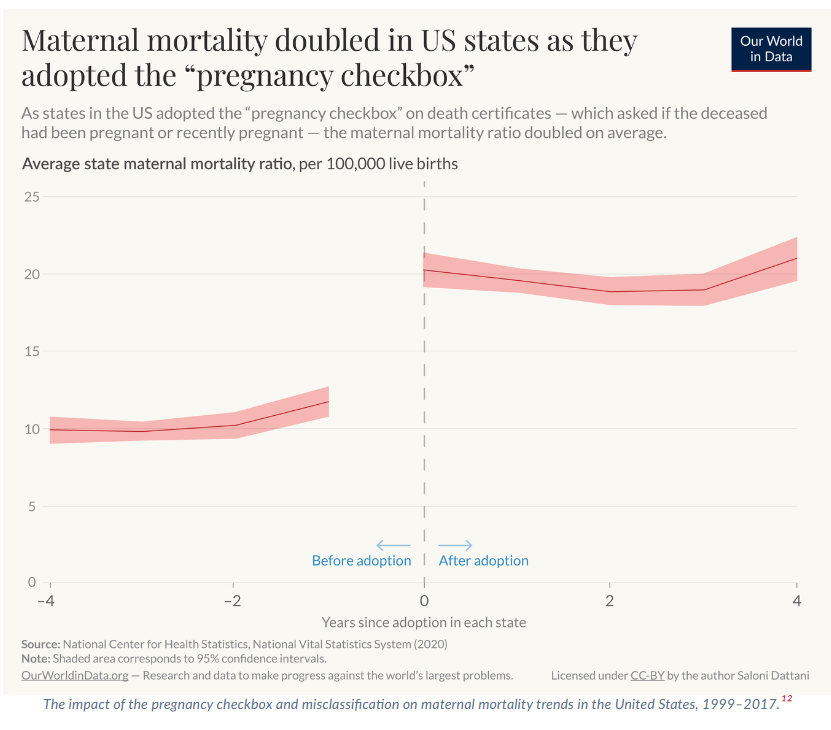
Joseph, et al, who wrote one of the most cited papers on this topic, estimate that the US maternal mortality rate is actually closer to 10.4 per 100,000 births (compared to the CDC’s estimate of 32.9 deaths per 100,000 births).
So what do we do with this information? While it could be interpreted as good news in many ways, it does not mean the issue should be dismissed. We cannot stress enough that the majority of maternal deaths are preventable, and that we must continue to advocate for increased mental health screenings, support with substance use, research into cardiac health during the pregnancy and postpartum period, and other aspects of the maternal/parental experience that tend to be overlooked. Additionally, accounting for the errors of the checkbox system does not change the fact that Black pregnant and parenting people have substantially higher rates of mortality. The work to combat these disparities should not end.
As youth-serving adults, we can do our part to help reduce racial disparities in healthcare by ensuring sex ed is comprehensive and intersectional, framing our conversations about bodily autonomy and access to healthcare in terms of systemic racism and an understandable distrust of the medical system by many people of color. And as access to vital reproductive healthcare continues to be attacked and restricted, we can help people get the care they need by supporting practical support organizations like Apiary and Gloria, reproductive justice initiatives, and legislation in our local communities that supports restoring reproductive rights.